
Radiology departmental precautions for Inpatient and ED patients with confirmed or suspected COVID-19 are the same. When clinically necessary, portable imaging will be the initial approach and any needed imaging in the department will follow protocol established by the department of Radiology and infection control.
You MUST read daily emails from Broadcast PHS and Broadcast Brigham for latest updates and changes to our policies and procedures on this rapidly developing priority.
- When COVID-19 is clinically suspected, portable chest radiograph will be the initial imaging study.
- Chest CT is NOT considered a screening test for COVID-19 at Brigham Health. Chest CT can be performed at the discretion of the referring clinical team and is generally reserved for patients with suspected complications, strong consideration for alternate diagnoses or severe level of illness (e.g. immunocompromised patients).
COVID-19, like any viral pneumonia, has a spectrum of imaging manifestations, ranging from normal chest CT to diffuse airspace disease in the setting of acute respiratory distress syndrome (ARDS). A collection of radiology literature may be found at Radiology’s website https://pubs.rsna.org/2019-ncov . We highlight two articles for reference of CT imaging appearance: Shi H, et al. Lancet Infectious Diseases 2020 (https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(20)30086-4/fulltext); and Bai HX, et al. Radiology 2020 (https://pubs.rsna.org/doi/10.1148/radiol.2020200823). These articles show that the typical imaging manifestations are of bilateral patchy ground glass opacities with peripheral distribution and lower lung predominance. In the early phase, subpleural, patchy or rounded ground glass opacities have been described and findings can be either bilateral or unilateral. Notably, bronchiolitis (centrilobular or tree-in-bud nodules) is not a typical manifestation, nor are pleural effusions.
We have included an example case taken from SIRM in Italy (https://www.sirm.org/2020/03/10/covid-19-caso-33/):
 |
 |
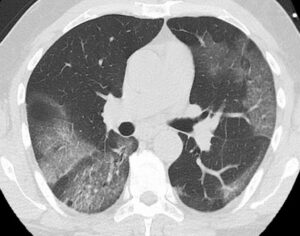 |
Please remember that, in the absence of clinical context and in a non-endemic area, the typical CT findings are nonspecific. They may reflect other viral pneumonias, inflammatory conditions such as organizing pneumonia, or other processes such as alveolar hemorrhage, pulmonary edema, or aspiration, depending upon the appearance.
Given the need to minimize exposure to patients with suspected or known COVID-19, consider the clinical reason for imaging in these patients, and if relevant, seek clarification before imaging is performed by evaluating the medical record or discussion with ordering/responsible provider to help reduce unnecessary or redundant exams. A new precautions column in Epic protocol worklist or in Epic snap boards, displays a red biohazard icon for COVID-19 confirmed and black biohazard icon for COVID-19 suspected patients.
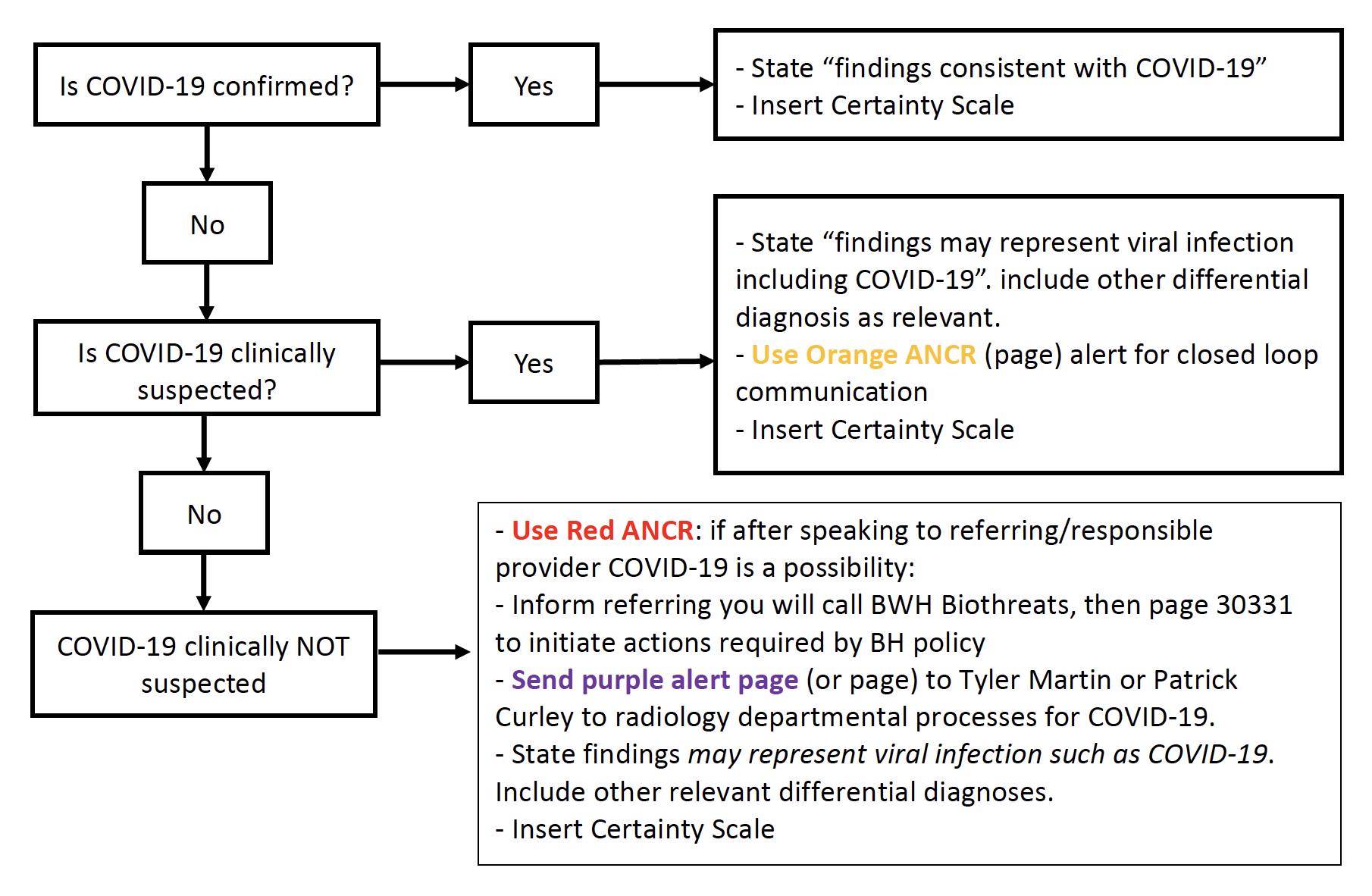
In the IMPRESSION of your radiology report (with typical imaging findings described above):
- If COVID-19 is already confirmed
- State that findings are consistent with COVID-19.
- Insert Certainty Scale at the bottom the report (powerscribe shortcut is type cs and press enter).
- If COVID-19 is clinically suspected
- State findings may represent viral infection such as COVID-19. Remember to include any other differential diagnoses, as appropriate, again using certainty terms.
- Use Orange ANCR (page) alert for closed loop communication with responsible or ordering provider.
- Insert Certainty Scale at the bottom the report (powerscribe shortcut is type cs and press enter).
- If COVID-19 is clinically unsuspected
- Use Red ANCR (page) for closed loop communication with responsible or ordering provider. If after discussion with ordering/responsible provider COVID- 19 becomes a possible diagnosis, you should mention COVID-19 specifically in your report using relevant certainty terms.
- Inform referring provider that you will contact Brigham Biothreats by paging 30331. This will initiate actions required by PHS/BH policy for COVID-19.
- Send purple alert page (or page) to Tyler Martin or Patrick Curley to initiate necessary radiology departmental processes for COVID-19.
- State findings may represent viral infection such as COVID-19. Remember to include other clinically relevant differential diagnoses in your impression.
- Insert Certainty Scale at the bottom the report (powerscribe shortcut is type cs and press enter).
- Use Red ANCR (page) for closed loop communication with responsible or ordering provider. If after discussion with ordering/responsible provider COVID- 19 becomes a possible diagnosis, you should mention COVID-19 specifically in your report using relevant certainty terms.
- If the imaging findings are that of a viral pneumonia but not typical for COVID-19, you simply report that “findings may/likely represent a viral pneumonia.”.
- if you have any questions about whether findings may represent COVID-19, you can consult thoracic radiology attending on call (or the reading room during the day). Consider using COVID-19 Consult option which has been set up in Worth Another Look (please page).
- if you have any questions about whether findings may represent COVID-19, you can consult thoracic radiology attending on call (or the reading room during the day). Consider using COVID-19 Consult option which has been set up in Worth Another Look (please page).
- DO NOT INCLUDE COVID-19 in your findings or impression other than scenarios 1-3 described above and be mindful that the absence of findings on imaging including Chest CT does not exclude COVID-19 infection.
Please email/call/page Patrick Curley or Ramin Khorasani with any questions.
Patrick Curley
Ramin Khorasani
Giles Boland
If Typical Imaging Findings Described Above:
If Imaging Findings of Viral Pneumonia or if Atypical for COVID-19:
- Use Orange ANCR (page) alert for closed loop communication
- State “findings may represent/likely represent viral pneumonia. Include other relevant differential diagnoses. DO NOT INCLUDE COVID-19 IN YOUR IMPRESSION
- Insert Certainty Scale
- If unsure consult thoracic radiology: use purple ANCR COVID-19 consult; or call reading room 617-278-5502 or page thoracic radiologist on call