
- Measure at site of most severe inflammation
- Avoid measuring nondistended bowel (may overestimate)
- Look for nodularity/mass-like thickening that may indicate malignancy
| Severity | Thickness |
|---|---|
| Mild | 3-5 mm |
| Moderate | 5-9 mm |
| Severe | ≧ 10 mm |
| Finding | Description | Pearls | Example |
|---|---|---|---|
| Segmental mural hyperenhancement | Different subtypes:
|
Avoid “mucosal hyperenhancement”; instead use “inner wall hyperenhancement” |  |
| Mural edema |
|
Should be assessed ONLY on T2FS; hyperintense T2 signal may be edema or mural fat, which is a sign of chronicity, unrelated to active inflammation |  |
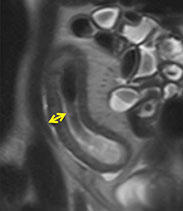
| Ulcerations |
|
Should not use term “penetrating ulcer”, so as not to be confused with penetrating disease |  |
- May show delayed post-contrast enhancement
- May be superimposed on active inflammation and penetrating disease
| Upstream dilatation | Severity |
|---|---|
| None (but multiple series shows fixed narrowing) | “Probable stricture present” |
| 3-4 cm | Mild |
| >4 cm | Moderate to severe *consider “SBO” |

Penetrating Disease
| Finding | Description | Example |
|---|---|---|
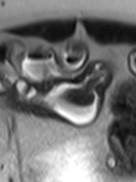
| Simple fistula | Single tract connecting 2 epithelial structures | 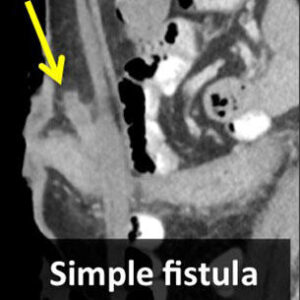 |
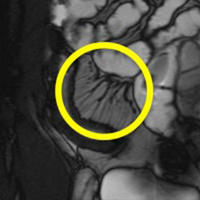
| Complex fistula | Multiple extra-enteric tracts, often asterisk- or clover-leaf-shaped | 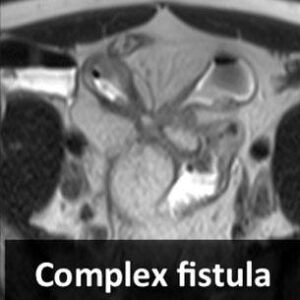 |
| Sinus tract | Tract that does not communicate with a second epithelialized structure | |
| Inflammatory mass | Ill-defined mass-like process (may contain mixed fat or soft tissue, but not water) *Should not use the term “phlegmon” | 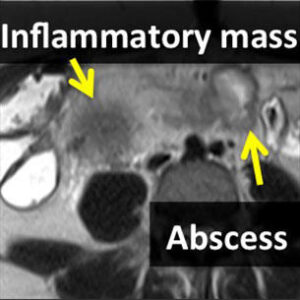 |
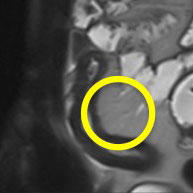
| Abscess | Fluid collection with rim enhancement |
*Note: Perianal disease is not considered penetrating disease
Ancillary Findings
| Ancillary findings | Description | Example |
|---|---|---|
| Restricted diffusion |
|
 |
| Perienteric edema |
|
 |
| Engorged vasa recta |
|
 |
| Fibrofatty proliferation |
|
 |
| Pseudosacculation |
|
 |
| Adenopathy |
|
| Category | Finding |
|---|---|
| MSK |
|
| GI |
|
| GU | Nephrolithiasis |
| Vascular | Mesenteric venous thrombosis/occlusion |
Bruining DH, Zimmermann EM, Loftus EV, Sandborn WJ, Sauer CG, Strong SA, Society of Abdominal Radiology Crohn’s Disease-Focused Panel. Consensus Recommendations for Evaluation, Interpretation, and Utilization of Computer Tomography and Magnetic Resonance Enterography in Patients with Small Bowel Crohn’s Disease. Radiology. 2018 Mar;286(3):776-799.